Course objectives
After completing the course, learners will be able to:
- Describe the implications for maternal and infant health during public health emergencies.
- Describe how Maternal and Child Health (MCH) and Public Health Emergency Preparedness and Response (PHEP) programs can collaborate to address population needs throughout the emergency management cycle.
- Identify discrete activities that promote the integration of MCH considerations in emergency preparedness and response plans.
Prerequisite knowledge and skills
- Interest in how to elevate and more equitably address maternal and infant health needs during all types of emergencies.
- Ability to navigate a web-based learning course with multimedia (video clips, .pdf documents, hyperlinks to external websites) and interactive (i.e., “try it”) components.
Intended audiences
This course is meant for people who: (a) work in or intersect with public health at any level of government, (b) are poised to influence outcomes for women of reproductive age, specifically pregnant and postpartum people, and infants, and (c) provide direct, enabling, or system-level support to communities during emergencies. After passing a summary post-test on the CDC’s TRAIN platform, course completers will be eligible for the following types of Continuing Education (CE) credit:
- Continuing education contact hours (CECH) in health education by the National Commission for Health Education Credentialing, Inc. for Certified Health Education Specialists (CHES®) and Master Certified Health Education Specialists (MCHES®)
- Recertification Credits by the National Board of Public Health Examiners for Certified Public Health Professionals (CPH)
- Continuing nursing education (CNE) contact hours through the American Nurses Credentialing Center
- International Accreditors for Continuing Education and Training Continuing Education Units (CEU) for all health professionals
Instructions
The modules in this course are intentionally sequenced to support learning; each module builds on content presented in the previous module. At points, you will be prompted to stop and complete reflection and/or application activities (e.g., action planning) in a participant workbook. This is an accessible, fillable .pdf document that you can save to your desktop, add to as you complete the course, and keep for later reference. While not required, the workbook promotes active engagement with course content and application of learning to your professional role(s).
Anticipated time to complete: 90 minutes
Module 1: Introduction
What are public health emergencies?
| A public health emergency is a natural or human-made event that negatively affects the health of a population and creates the conditions for widespread illness or disability. Public health emergencies disrupt lives, families, and communities. They fall into three categories: natural disasters, such as hurricanes, tornadoes, wildfires, floods, and earthquakes; Emerging or significant outbreaks of diseases, such as Covid-19, Zika virus, Ebola, and pandemic influenza; and human-caused disasters, such as nuclear accidents, bioterrorist attacks, and war. |  |
| For any public health emergency, there are four cyclical and recurring phases of management: mitigation, preparedness, response, and recovery. | 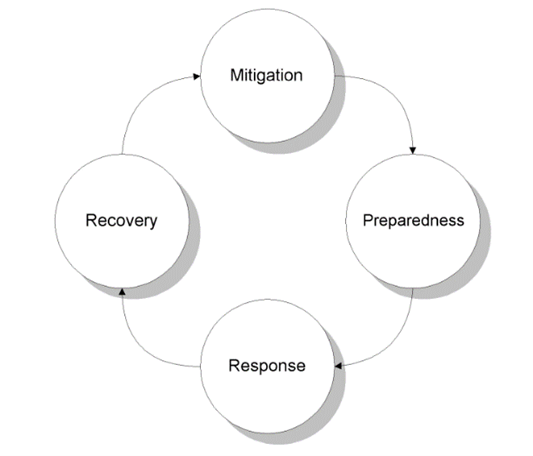 |
Mitigation: Actions taken to prevent and reduce the overall cause and impact of disasters including, but not limited to: constructing levees or other permanent barriers to control flooding, tying down buildings with ground anchors to withstand high winds, and buying insurance policies.
Preparedness: Planning, training, and education for disaster events that cannot be mitigated or prevented, such as participating in disaster drills and tabletop exercises, and developing preparedness plans for what to do in case of a disaster.
Response: Actions taken in the duration or immediate aftermath of a disaster, including implementing disaster response plans, addressing public health concerns such as disease spread and food contamination, and conducting search and rescue missions.
Recovery: Efforts occurring when regular operations and activities are re-established. The recovery period can often be prolonged and includes activities such as preventing or alleviating financial burden, rebuilding damage structures, and starting mitigation activities to lessen vulnerability during future disasters.
Why focus on women of reproductive age, specifically pregnant and postpartum people, and infants?
In this video clip (3:38), Dr. Wanda Barfield, Director of the Division of Reproductive Health at the CDC, addresses the importance of centering women of reproductive age – specifically pregnant and postpartum people, and infants – in emergency preparedness and response. She provides poignant examples of successes and unique challenges for these populations that surfaced during multiple types of recent emergencies.
Other reasons why we choose to center these populations include:
- Federal legislation identifies pregnant and postpartum women and infants as populations with special clinical considerations in public health emergencies;
- People who are pregnant or postpartum may experience higher rates of poor reproductive outcomes during and after disasters, such as miscarriages, premature deliveries, cases of intrauterine growth restriction (IUGR), low birth weight infants, sexual violence, and lack of access to contraception2;
- Pregnant, postpartum, and breastfeeding people and infants may be uniquely impacted by public health issues resulting from disasters, such as contaminated food and water sources2; and
- Focusing on the specific circumstances experienced by birthing people and infants contributes to an “all hazards approach” by ensuring that health and other systems have the capacity to address the broadest possible range of emergency needs. This includes preventing excess adverse outcomes and exacerbations of existing health disparities in pregnancy-related morbidity and mortality.
How can preparedness and response activities be platforms for evidence-based, equity-centered practice?
Disasters occur within a specific context based on a community’s geographic, cultural, demographic, political, and historical characteristics, which produce unique considerations for each1. They require tailored solutions. As an example, the Stafford Act requires FEMA assistance be delivered in an equitable manner without discrimination on the grounds of race, color, religion, nationality, sex, age, disability, language accessibility, or economic status. However, this cannot be done through a one-size-fits-all approach.
Executive Order 13985 (January 20, 2021) defines equity as “the consistent and systematic fair, just, and impartial treatment of all individuals, including individuals who belong to underserved communities that have been denied such treatment, such as Black, Latino, and Indigenous and Native American persons, Asian Americans and Pacific Islanders and other persons of color; members of religious minorities; lesbian, gay, bisexual, transgender, and queer (LGBTQ+) persons; persons with disabilities; persons who live in rural areas; and persons otherwise adversely affected by persistent poverty or inequality.”
Watch this video clip (2:30) that describes the critical need to apply equity frameworks across all phases of emergency management. This perspective is reinforced by federal entities, such as the Federal Emergency Management Agency (FEMA). Pages 9-13 of their strategic plan identifies opportunities to “instill equity as a foundation of emergency management,” such as:
- Understand the factors that affect a community’s resilience and vulnerability to disasters;
- Proactively and continuously engage state, local, tribal, and territorial partners, local community leaders, and other community representatives to gain insight into how programs can better serve them;
- Make space to invite and elevate diverse voices, and to foster mutual understanding and respect for [different] perspectives and experiences;
- Deliberately [define] what success looks like for each user of each program in a manner that can be consistently measures;
- Routinely evaluate programs and policies for disparities in outcomes; and
- Conduct ongoing equity-based evaluations across programs, as well as partner with external organizations experienced in this work.
Module 2: MCH and PHEP 101
Public Health Emergency Preparedness (PHEP)
This video clip (6:22 of total content) was excerpted from a presentation delivered by Gerrit Bakker, the former Senior Director of Preparedness at the Association of State and Territorial Health Officials (ASTHO). It aims to establish a baseline of understanding about the critical role that PHEP has played and can play in addressing maternal and infant health priorities before, during, and after emergencies. Topics covered in the video clip include:
- The origins of PHEP in the United States
- What prompted the development of the PHEP Capabilities
- The legislative underpinnings of PHEP
- Pandemic and All-Hazards Preparedness Act (PAHPA)
- Public Health Emergency Preparedness Program (CDC)
- Hospital Preparedness Program (HHS/ASPR)
- Health department responsibilities for capacity building within the PHEP capabilities
- Emergency response infrastructure at each level of government
Maternal and Child Health (MCH)
This video clip (8:55) aims to establish a baseline of understanding about the services and systems (specifically those established by Title V of the Social Security Act) that specifically address the health needs of women, children, and families. It provides critical information about and access points for these special populations in preparing for and responding to emergencies. Presenter: Ben Kaufman, Associate Director for Workforce Development and Capacity Building, AMCHP.
Critical Intersections
The following video clips (7:03 of total content) were excerpted from a presentation delivered by Romeo Galang, MD, MPH, Medical Director, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. This team aims to establish women of reproductive age, especially pregnant and postpartum people, and infants as priority populations in all phases of the emergency management cycle.
| What are the disaster effects and concerns specific to women of reproductive age, pregnant and postpartum people, and infants in public health emergencies? | Start at 6:07 and end at 12:31 |
|
Why is it important to integrate EPR and maternal and infant health (MIH) at the jurisdictional level?
|
Start at 15:19 and end at 15:58 |
WATCH: This video clip (4:47) connects gains in individual knowledge, skills, and abilities to collective emergency response capability. It references two federal guidance documents from the fields introduced above that learners are encouraged to explore in greater depth. Presenter: Mikayla Frye, Program Manager for Workforce Development and Capacity Building, AMCHP.
- Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health, 2018 Update (Centers for Disease Control and Prevention)
- Maternal and Child Health Leadership Competencies, Version 4.5 (Health Resources and Services Administration)
Supplemental Resources
| Title | Author(s) | Format | Purpose |
| Reproductive Health in Emergency Preparedness and Response | CDC | Informational page (link) on a federal website. | Gain a better understanding of the role that DRH plays in facilitating effective responses |
| Public Health Emergency Preparedness and Response Capabilities | CDC | Informational PDF (link) on a federal website. | Summaries of each of the 15 PHEP capabilities are available on pages 11-18 |
| Office of Readiness and Response (ORR) Website | CDC | Interactive page (link) on a federal website. | Provide access to the most current information about efforts to advance preparedness and response efforts. |
| MCH Timeline | HRSA – Maternal and Child Health Bureau | Interactive page (link) on a federal website. | Trace the history of maternal and child health in the U.S. and orient those new to the profession. |
| Title V Information System (TVIS) | HRSA – Maternal and Child Health Bureau | Federal website (link) with data visualizations and multiple interactive components. | Provide detailed information about maternal and child health priorities, investments, and outcomes within and across U.S. jurisdictions. |
| Lessons Learned from Public Health Emergencies | Dr. Sascha Ellington, former CDC team lead | Video clip (3:27) from a recorded webinar. | Briefly highlight lessons learned for maternal and infant health from the Zika, H1N1, COVID-19 responses. |
Learning Check: Module 2
Based on what you’ve learned, answer the following multiple-choice questions. When you click “submit,” you will see which of your responses were correct. For those questions you answered incorrectly, the correct answer will also be visibly indicated. For all questions, a brief statement justifying the correct answer will be provided.

| Who in your jurisdiction is poised to influence outcomes for MCH populations during emergencies? The Reflection Activity on pages 1-2 of the participant workbook (see beginning of this course to download the fillable .pdf document) prompts you to conduct a brief landscape/ecosystem analysis and draft talking points that are specific to people you’ve identified as important. |
Module 3: The Public Health Emergency Preparedness and Response Checklist for Maternal and Infant Health
Originally designed to guide interdisciplinary teams from U.S. states, territories, or freely associated states participating in AMCHP’s Emergency Preparedness and Response Action Learning Collaborative, this Checklist is intended to augment the capacity of all jurisdictions to ensure that women of reproductive age, especially pregnant and postpartum people, and infants are planned for in the event of emergencies – including multiple emergencies with intersecting impacts. This tool was repeatedly recognized by participants as a useful tool for prioritizing strategies and selecting action items.
In this video clip (8:53), Dr. Marianne Zotti provides an overview of the Checklist that includes background, alignment with federal emergency preparedness guidance, a brief description of the four overarching strategic areas, and how to read and use each Checklist component.
Later in the course, you will complete reflection and application activities that require you to interact with both the Checklist and Action Item Cards (the structure of these are described beginning at 7:51 of the previously referenced video clip) that elaborate on planning and implementation considerations associated with each activity. You will be able to “jump” to and from these as you complete the activities using the workbook, but it is recommended that you download these for easy access.
Module 4: Integrate MCH Considerations into the Jurisdiction Emergency Preparedness and Response Plan (Checklist Strategy #1)
Before starting this module, make sure you’ve downloaded and/or printed both the Checklist and Action Implementation Cards for easy reference.
Overview
This video clip (2:30) introduces the upcoming presenters and offers a “big picture” perspective on the significance of this strategy in building overall preparedness and response capacity. Presenter: Ben Kaufman, Associate Director for Workforce Development and Capacity Building, AMCHP.
Activities within Strategy #1 support three (3) PHEP capabilities:
- Community Preparedness
- Mass Care
- Emergency Operations Coordination
Didactic Breakdown of Select Activities
Watch the following video clips to learn about a few activities included in the checklist for Strategy #1. You can find the complete list of Checklist activities that support Strategy #1 in the Checklist document offered for download at the start of this course.
| PHEP Capability | Activity | Presenter | Length | Selection Rationale | Play Video |
| Community Preparedness | S1-A2. Are lists of key jurisdictional MCH partners, stakeholders, and/or social networks updated annually to reflect current contact information? | Marianne Zotti, DrPH, FAAN Emeritus | 0:35 | Many subsequent activities hinge upon thoughtful selection and engagement of partners. | |
| Community Preparedness | S1-A3. Is an MCH staff member identified who regularly reviews and updates the sections of the jurisdiction plan that pertain to MCH populations? If yes, who? | Marianne Zotti, DrPH, FAAN Emeritus | 0:44 | Plan awareness and review is foundational for integrating and ultimately operationalizing population-specific considerations. | |
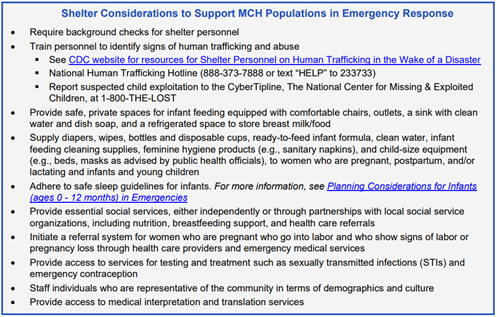
| Mass Care | S1-A4. Does jurisdiction guidance for sheltering and other mass care address maternal and infant population-specific needs, such as supplies and instructions for infant feeding and safe sleep? | Marianne Zotti, DrPH, FAAN Emeritus | 1:29 | Speaks directly to a situation-specific application of population needs. | |
| Emergency Operations Coordination | S1-A6. Has staff evaluated the MCH role in the last jurisdiction response where the hazard had a disproportionate effect on women of reproductive age and/or infants (such as Zika virus or pandemic influenza)? | Amy Moskovitz, MPH, CLC | 0:43 | Prompts critical thinking about previous emergencies and how to use After Action Reports to inform future efforts. | |
| Emergency Operations Coordination | S1-A7. Has your MCH Program defined how MCH staff become EPR trained and response-ready? | Amy Moskovitz, MPH, CLC | 1:54 | Addresses multiple levels (individual, departmental, organizational) of accountability. |
Centering Equity in Practice
Addressing maternal and infant health needs in planning for and responding to emergencies cannot be disconnected from the broader pursuit of equitable outcomes for all. This video clip (2:00) demonstrates how to apply an equity lens in implementing a specific capacity building activity (S1-A2). A primary takeaway is that intentionally engaging diverse partners is critical for ensuring that equitable processes are guiding implementation of all Checklist activities. Presenter: Ben Kaufman, Associate Director for Workforce Development and Capacity Building, AMCHP.
Voice from the Field
WATCH: In this video clip (2:42), Erika Fuchs, the CDC’s MCH Field Epidemiology assignee to the Nebraska Department of Health and Human Services, shares her experiences collaboratively leading state efforts to operationalize S1-A3. This includes details regarding the types of plans that were sought and reviewed, how the review process was structured and shared among team members and plans for communicating consensus MIH priorities with leaders in charge of specific emergency operations.
Implementation Support Spotlight: Sheltering
Mass Care is a topic that is often included in preparedness exercises and jurisdictional EPR plans. The two resources below can help learners elevate MIH considerations in specific contexts that pregnant and postpartum people and infants frequently need to navigate during emergencies. They are especially relevant to S1-A4. Even if you are not working directly in shelters, consider how you may be positioned to make these ideal conditions possible.
REVIEW: The graphic below, “Shelter Considerations to Support MCH Populations in Emergency Response,” can be found on page 26 of the HHS Maternal-Child Health Emergency Planning Toolkit (link).
EXPLORE: The “Supporting Optimal Infant and Young Child Feeing in Emergency Shelter Settings” section of the CDC’s Infant and Young Child Feeding Toolkit (link) provides practical guidance for emergency shelter personnel during the preparation and response phases.
Implementation Support Spotlight: Training
This brief list of EPR training resources below was compiled by AMCHP and is relevant to S1-A7. These courses and toolkits were recommended based on the credibility of their sources and their potential to advance either: (a) individual knowledge development or (b) organizational capacity.
| Title | Author(s) | Format |
| Independent Study Program (ISP) Course List | Federal Emergency Management Institute (FEMA) | Webpage that lists a range of free, asynchronously accessible emergency training courses including Introduction to the Incident Command System (ICS-100) and Introduction to the National Incident Management System (IS-0700.b). |
| HHS Maternal-Child Health (MCH) Emergency Planning Toolkit | Assistant Secretary for Preparedness and Response (ASPR) | Document that outlines basic planning steps, highlights key resources and promising practices, and explains critical data and information to be integrated into MCH planning for MCH populations. Four case studies are provided. |
| Emergency Preparedness and Response Training for Public Health Epidemiologists | Council of State and Territorial Epidemiologists (CSTE) | Course and accompanying workbook to increase capacity for epidemiologists’ participation in large scale outbreaks, emergency activations, and/or other emergency preparedness and response activities. |
| Disaster Preparedness: Pediatric Tabletop Exercise Resource Kit | American Academy of Pediatrics (AAP) | Webpage that includes tools (e.g., agendas, email invitations, follow up work) needed to plan and implement a tabletop exercise, as well as an extensive list of case scenarios. |
Learning Check: Module 4
Based on what you’ve learned, answer the following multiple-choice questions. When you click “submit,” you will see which of your responses were correct. For those questions you answered incorrectly, the correct answer will also be visibly indicated. For all questions, a brief statement justifying the correct answer will be provided.
Thank you for completing this course! We hope the content met or exceeded your expectations for learning and that the interactive components will support your readiness to champion maternal and infant health needs in preparing for and responding to future emergencies.
To receive continuing education (CE) credit for this course, click the button below to be directed to the CDC TRAIN platform where you will complete a brief post-test (and create a free account if you have not already registered for one). You must score 80% to pass and will only be allowed one retake.
Please contact workforce@amchp.org with any questions about the course or feedback for the architects.
| Where should my organization/agency start? What’s my role? The Application Activity on pages 3-4 of the participant workbook (see beginning of this course to download the fillable .pdf document) prompts you to use an impact matrix tool to select a priority activity within Checklist Strategy #1 and determine individual action steps. The red buttons at the top right of each page are links to documents that can support your decision making. |