AMCHP partners with community-rooted organizations, Title V programs, governmental and private funders, and fellow non-governmental organizations to support our members in creating maternal and infant health initiatives that center racial equity. We do this by creating projects that encourage our members to think critically about how racism impacts perinatal, birth, and infant health outcomes. We administer compassionate and equity-centered learning collaborative spaces that feature thought leaders in the space of perinatal health, maternal health, birth equity, and reproductive justice where we challenge our members to address racism as the root cause of health inequities.
We seek and celebrate collaborative, equitable partnerships with community-rooted organizations to connect our members to their expertise for mutually beneficial relationships. Through our Maternal and Infant Health initiatives, we find creative ways to celebrate the successes of our members, while finding new ways to support their growth in dedication to racial equity.
Current Initiatives
- Support for Maternal Mortality Review Committees
- Safer Childbirth Cities Initiative
- Alliance for Innovation on Maternal Health (AIM)
- Healthy Beginnings with Title V
- State Level Support for Maternal Health and Early Child Feeding: Birth to 2 Years
AMCHP’s Women’s and Infant Health team is happy to support the Enhancing Reviews and Surveillance to Eliminate Maternal Mortality (ERASE MM) project administered by the Centers for Disease Control and Prevention (CDC). Through our partnership with the CDC, Maternal Mortality Review Committees (MMRCs) from various state and local governments are supported with consistent and comprehensive resources and tools to decrease and eliminate preventable maternal deaths. Our flagship project, ReviewtoAction.org serves as the lead resource and networking tool for these MMRCs.
ReviewtoAction.org features elements to learn the basics of MMRCs and their purpose, practice via webinars and trainings on reviewing maternal deaths, and implement guidelines and recommendations to decrease the prevalence of maternal mortality. From national resources on setting up an MMRC to state legislation on the authorities of MMRCs, a multitude of resources can be found on ReviewtoAction.org for the open public and MMRCs members.
In addition, we assist in hosting the annual gathering for MMRCs members for training in the review systems of maternal deaths, MMRIA (Maternal Mortality Review Information Application). In these annual meetings, called MUMs (MMRIA User Meetings), MMRC members not only receive training on the user application, but also on implicit bias, health equity, and community inclusion and collaboration. The graphic and video recordings of these meeting sessions are available on ReviewtoAction.org.
We look forward to developing webinars and additional resources for those looking to center health equity, anti-racism, and community leadership in the work to eliminate maternal mortality.
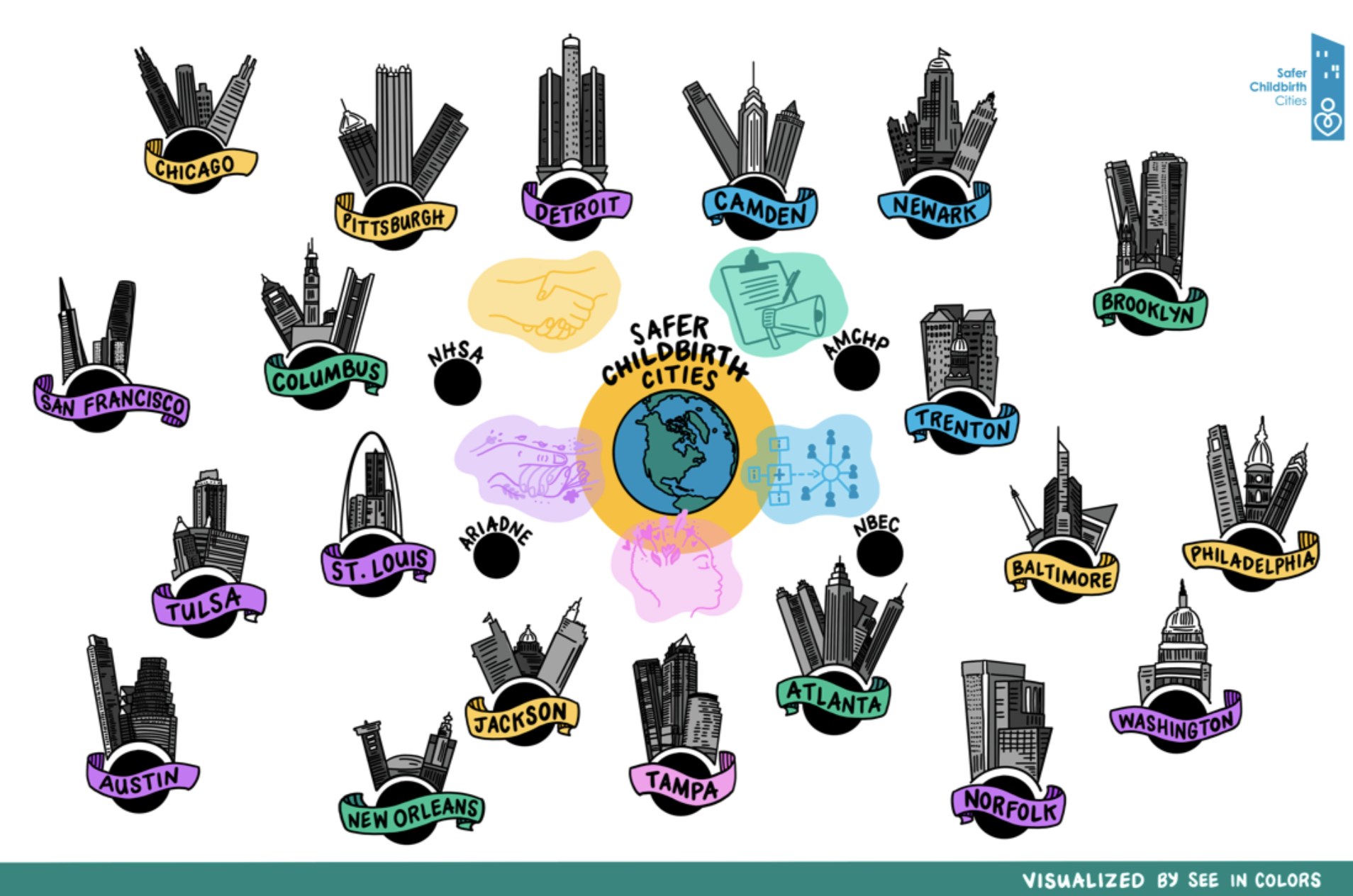
The Safer Childbirth Cities Initiative (SCC) supports community-based organizations in U.S. cities with a high burden of maternal mortality and morbidity in their implementation of evidence-based interventions to reverse the country’s maternal health trends. Currently, 20 cities have been funded. Cohort 1 includes Atlanta, Baltimore, Camden, Chicago, Columbus, Jackson, Newark, New Orleans, Philadelphia, and Pittsburgh. Cohort 2 includes Austin, Brooklyn, Detroit, Norfolk, St. Louis, San Francisco, Tampa, Trenton, Tulsa, and Washington, DC.
The Association of Maternal and Child Health Programs (AMCHP) was funded to host a Community of Practice to foster a space of support, problem solving, and celebration as each organization implements their work. AMCHP provides technical assistance and capacity building in high-priority focus areas that were collectively identified with each city-based team. Efforts of the SCC grantees are centered on a range of focus areas including maternal mental health, doula support, trauma-informed care, data informatics and health information systems. The work of the grantees illustrates the importance of addressing perinatal and family health inequalities with a racial equity lens and centering the communities each program intends to serve.
Centering Patient Voices on Quality Improvement
In Fall 2018, AMCHP became an Executive Team member of the Alliance for Innovation on Maternal Health, or AIM, joined by fellow national and state organizations working to address maternal morbidity and mortality in the nation. American College of Nurse-Midwives (ACNM), the Association of Women’s Health, Obstetric, and Neonatal Nurses (AWHONN), the National Perinatal Information Center, Society for Maternal-Fetal Medicine, and the California Maternal Quality Care Collaborative. Since 2014, AMCHP has been a core partner on this initiative, which is a cooperative agreement between the American College of Obstetricians and Gynecologists (ACOG) and HRSA-MCHB to implement a national data-driven maternal safety and quality improvement initiative. AIM works through state and community-based teams to align national, state, and hospital level quality improvement efforts to improve overall maternal health outcomes. As an Executive Team member, AMCHP is responsible for evaluating the enrollment of new states into the AIM initiative, advising programmatic decision-making, and especially in the case where a Title V/MCH program is taking a lead role in state AIM implementation, attending the in-person kick-off meetings of the state, and supporting implementation of AIM in that state as needed.
Test of Integration of the Reducing Peripartum Racial & Ethnic
In 2018, Northwell Health’s Long Island Jewish Medical Center (LIJMC), Ancient Song Doula Services (ASDS), and Public Health Solutions (PHS), in collaboration with the Association of Maternal and Child Health Programs (AMCHP) entered a test of integration of the Reducing Peripartum Racial & Ethnic Disparities bundle. A co-author of this bundle, AMCHP is invested in learning the obstacles to its implementation and the impact it can have in the clinical space. Over time, this test of integration has transformed in alignment with the efforts of the AIM program, to focus on centering respect for the birthing person and racial equity in all aspects of maternity care quality improvement. While the test of integration continues to focus on aspects of RPRED bundle implementation, it is more foundational in its approach. In the test of integration, community partners helped identify three main pillars for advancement and improvement:
- The conceptual versus the practical. While the RPRED bundle helps users conceptualize the issue of racial and ethnic disparities, the bundle does not provide practical guidance and instruction to address said disparities. For example, the bundle suggests hospitals “build a culture of equity,” however, does not provide how institutions are to do so.
- Centering community voices. The bundle does not provide space for the experiences of people of color who interact with the hospital system, specifically Black and Indigenous peoples from the communities served. In equity work, it is important to pull from the margins to center the voice, experiences, and knowledge of those who traditionally have been excluded. However, the bundle does not provide guidance, conceptual or practical, for hospitals and clinical sites on how to engage with local communities of color in this way.
- Lack of accountability. A key component missing from the bundle is how to develop and implement a system of multi-level accountability. To fully address the racial and ethnic disparities, the disparate data need not only to be identified, but the mechanisms that cause the outcomes to persist need to be analyzed and appropriately held accountable. This accountability not only needs to occur at a provider-patient level, but at the administrative, insurance, and community levels.
The program team continues to build out these pillars through transparent community engagement to develop and implement an accountability process designed specifically for the LIJ community served that promotes accountability not only between the hospital and patients served, but between clinicians and administration. Presently they are working to develop a toolkit documenting their process as well as continuing the process of transparently listening to the patients to develop accountability processes.
Phase I: Healthy Beginnings with Title V: Preterm Birth Priming and Planning
AMCHP and birth equity thought leaders developed resources and held conversations to uncover the unique power and flexibility of the Title V MCH Services Block Grant to pull intention and resources related to preterm birth prevention (and improving maternal and infant health outcomes generally) deeper into the roots of racial injustice. Through four webinars and issue briefs, we identified ways to achieve mom-baby dyad wellness by centering health equity and community co-creation in every step of the program planning cycle. This included understanding the root causes of racial disparities in preterm birth across the country and by race and geography, supporting emancipatory community engagement in data inquiry, analysis, and translation, and forming equitable partnerships with community-based organizations as the foundation for efforts that advance health equity in birth outcomes. The final webinar and issue brief concludes by highlighting recommendations of actions that Title V programs can take to partner with Black-women led community-based organizations leading in achieving holistic community wellbeing. During this partnership, AMCHP also convened a national meeting of public health, health care, and community thought leaders and institutional partners with a role in preterm birth prevention. Participants in the meeting created recommendations for embedding anti-racism into Title V policies and structures as an essential process to achieve a collective vision: Every parent and baby has the optimal conditions, support, and agency to arrive at full-term, ready to thrive every time.
The COVID-19 pandemic highlights the urgency to adopt racial equity-centered approaches. The disproportionate and unjust impact of COVID-19 on communities of color is a direct result of decades of public health and governmental policies that concentrate advantage in White communities. Governmental public health institutions operate predominantly from a White racial frame, and as a result, most programming and resource allocation is based on White racial dominant narratives and biases. This project sought to intentionally identify ways that Title V programs can transfer power to communities most impacted by inequitable governmental and public health policies.
Resources:
- Engaging the Power of Title V for Equity in Preterm Birth Prevention Issue Brief Series
- Engaging the Power of Title V to Understand and Intervene in Preterm Birth Webinar Series
Phase II: Healthy Beginnings with Title V: Advancing Anti-Racism in Preterm Birth Prevention
The Association of Maternal & Child Health Programs (AMCHP), with support from the Pritzker Children’s Initiative (PCI) and the W.K. Kellogg Foundation, is providing capacity-building assistance and support to state MCH and local birth justice organizations to build transformational partnerships, dismantle policies and programs that perpetuate racism through inequities in funding, and support the investment in, and sustainability of community solutions that protect birth outcomes of Black, Indigenous, Hispanic/Latine/x, Asian, Pacific Islander, and other birthing people of color. AMCHP will convene six teams comprised of state MCH agencies and community-based organizations, Tribal governments, and Tribal organizations in an 18-month Learning and Practice cohort. The cohort will identify and address racism in policy, data, and funding structures at the state level that sustains inequities in perinatal health, including preterm birth.
Learn more about the Healthy Beginnings Project and access our Learning Bundles
AMCHP developed the learning module “Understanding the Impact of Historical Racism on Early Child Nutrition” as a critical primer to a series of modules about how Title V staff can holistically incorporate early child nutrition into their work. The learning module can be complete here:
Understanding the Impact of Historical Racism on Early Child Nutrition
AMCHP, in partnership with the Association of State Public Health Nutritionists (ASPHN) and the United States Breastfeeding Committee (USBC), developed a series of learning modules for Title V staff about how to holistically incorporate early child nutrition into Title V work. The modules share key concepts and definitions in early childhood nutrition and introduce the Policy Systems and Environmental Change Framework. In the remaining three modules, each lever within the framework is illustrated using examples of efforts supported by state Title V programs or implemented by community-rooted organizations. Users engage in key concepts through interactive imagery, videos of example efforts, and knowledge checks. They are intended to provide Title V programs with new ideas and inspiration on how to be a critical partner to communities for positive and equitable impact in early child nutrition.
The learning modules “Integrating Early Child Nutrition into Title V: Building the Foundation”, “Changing Policies: Institutionalizing Positive Nutrition Support”, “Changing Systems: Improving the Nutrition Network for Infants and Toddlers”, and “Changing the Environment: Increasing Access to Nutritious Foods” were supported by the Centers for Disease Control and Prevention of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $200,000 with 100 percent funded by CDC/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, or the U.S. Government.
The content for these modules was developed by AMCHP in partnership with ASPHN and USBC. Please see full partner information below. The AMCHP Women’s and Infant Health team would like to thank ASPHN and USBC for their partnership in this project, and Sophia Hurr for her support developing the learning modules. AMCHP would also like to thank Healthy Start, Inc. Pittsburgh, Indigenous Peoples Task Force, and Martha’s Table for sharing their expertise in these modules. Finally, we would like to thank our members and their partners in the Ohio Department of Health, Wisconsin Department of Health Services, and DC Health for sharing their examples of integrating early child nutrition into their work.
Founded in 1952, The Association of State Public Health Nutritionists (ASPHN) is a non-profit membership organization that provides state and national leadership on food and nutrition policy, programs and services aimed at improving the health of our population and committed to advancing health equity through public health nutrition leadership. ASPHN’s membership is composed of more than 600 public health nutritionists located throughout all 50 states, the District of Columbia and five U.S. territories. ASPHN’s vision is “healthy eating and active living for everyone.” You can find ASPHN on the web at www.asphn.org and on Facebook at www.facebook.com/asphn.
The U.S. Breastfeeding Committee is a coalition of more than 100 organizations that support its collective mission to drive collaborative efforts for policy and practices that create a landscape of breastfeeding support across the United States. Its membership includes national, state, community, tribal, and cultural organizations throughout the nation, all coming together to protect, promote, and support human milk feeding as a public health imperative. You can find USBC on the web at http://www.usbreastfeeding.org.
Unveiling of the Perinatal Substance Use Special Issue in the Maternal and Child Health Journal
Almost one in four pregnancy-related deaths is attributed to mental health conditions, including substance use disorder (SUD), making them the leading underlying cause of pregnancy-related deaths. This special issue of the Maternal and Child Health Journal builds on the evidence base, with 21 open articles that feature the latest research, program, and policy initiatives in perinatal SUD. The special issue is sponsored by the Association of Maternal & Child Health Programs and the Association of State and Territorial Health Officials, with funding from the Maternal and Child Health Bureau within the U.S. Health Resources and Services Administration. We invite you to read the special issue (https://bit.ly/MCHJPerinatalSUD) and promote the special issue using AMCHP's social media toolkit (https://bit.ly/MCHJSocialMediaToolkit). Read More

Advancing Perinatal Substance Use Policy with People with Lived Experience – Webinar September 2023

Perinatal Substance Use: National and State Public Health Strategies
AMCHP & ASTHO hosted a webinar on March 27th featuring The White House Office of National Drug Control Policy (ONDCP). ONDCP shared its priorities for improving maternal health outcomes and expanding access to evidence-based treatment for perinatal populations, as outlined in two reports: (1) Substance Use Disorder in Pregnancy: Improving Outcomes for Families and (2) Model Substance Use During Pregnancy and Family Care Plans Act. The presentation also included recommendations and opportunities to strengthen local MCH behavioral health systems based on lessons learned from Vermont’s CHARM (Children and Recovering Mothers) Program. Read More
